60yr old female with fever and loss of appetite .
ICU BED 1

 PERIORBITAL CELLULITIS
PERIORBITAL CELLULITIS
 CORNEAL CONGESTION AND ECCHYMOSIS+
CORNEAL CONGESTION AND ECCHYMOSIS+
 Hourly monitoring chart:
Hourly monitoring chart:


 OPHTHALMOLOGY OPINION WAS TAKEN IN VIEW OF RIGHT ORBITAL CELLULITIS.
OPHTHALMOLOGY OPINION WAS TAKEN IN VIEW OF RIGHT ORBITAL CELLULITIS.

 DAY SOAP NOTES
DAY SOAP NOTES
 USG:
USG:

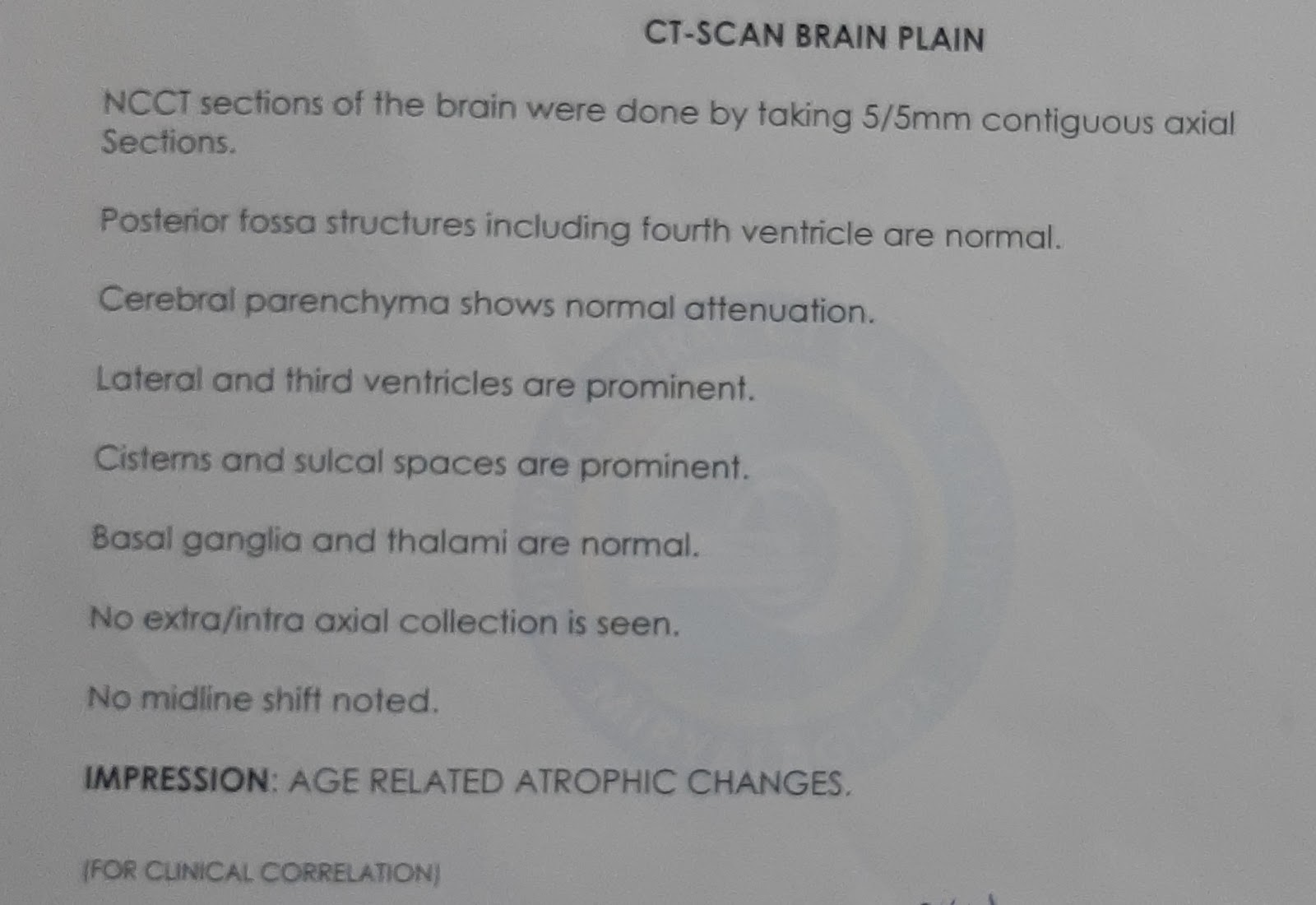
 LEFT PONTINE INFARCT
LEFT PONTINE INFARCT
60year old female who is home maker by occupation was diagnosed with diabetes since 10 years , intially used Oha and later shifted to insulin due to uncontrolled sugars.
Last year MARCH -2021 - H/o trauma , cellulitis and amputation was done in view of diabetic foot .
Last year May 2021- H/o ?CVA - Left hemiparesis with bowel and bladder incontinence. Pt is on Foley's since then.
Every 15 days they used to change it.
She got admitted in our hospital only during that time(documentation not available) and her weakness improved over 1 month and she was able to hodl things. But bladder incontinence still persisted .So she was on Foley's/diaper since then.
Cause could be -? aca territory infarct
Pt is bedridden since amputation and CVA .
No difficulty in speech or swallowing. She used to be active as per attenders.
She is not using her regular insulin since post CVA . She dint use any other medications since 8 months. Stopped antiplatelets also .
H/o fever 3 days ago- one episode.Loss of appetite was also there.
Since 2 days she had itching of her eyes and on repeated scrating , she developed redness and swelling of right eye .
No h/o ear pain, headache ,cold ,cough .
Since one day h/o altered sensorium and they got her to our hospital .
TEMP: AFEBRILE
PR-103bpm
BP-90/60mmJg
Rr- 30cpm
P/A - soft.
R/S-BAE +
CVS-S1 S2 +
CNS :Her GCS - currently is E3V1M3.
Pupils b/l not reacting to light. Mid dilated
R Eye - ptosis ,chemosis , redness present .
No EOM movements on right side. (opthalmoplegia).
Left eye - Pupil also not reacting to light .
No ptosis.
Right ear - Active discharge was coming out of External auditory canal today evening while examining .
Motor examination :
Power - couldn't be elicited as pt was altered .
Reflexes -
B. T. S. K. A. P
R. +2. +2. +1. +2. -. -
L. +2. +2. +. (amputated)
Tone - Left - hypotonia
Right -UL AND LL - NORMAL TONE.
Her Right eye opthalmoplegia can be secondary to local cause sir - ? orbital cellulitis with ear infection.
It could've even spread to cavernous sinus causing ?? cavernous sinus thrombosis .ú
Infection Will explain cause for DKA also .
X RAY CHEST
PROVISIONAL DIAGNOSIS: DKA SECONDARY TO ? NOT COMPLIANT TO MEDICATIONWITH HYPOVOLEMIC SHOCK SECONDARY TO DEHYDRATION(RESOLVED) WITH METABOLIC ACIDOSIS SECONDARY TO DA AND CKD RESOLVED H/O DM II CVA WITH LEFT AMPUTATED LEG ? WITH SEPTIC ENCEPHALOPATHY WITH RIGHT EYE ORBITAL CELLULITIS WITH RIGHT EAR ASOM
RX:-
1.IVF NS @ 150ML /HR.
2.INJ. 0.1 UNITS /KG/WT ACTRAPID IV/STAT.
3. INJ. PIPTAZ 2.25GM IV/TID.
4.INJ. ZOFER 4MG IV/SOS
5. INJ. PANTOP 30MG IV/OD.
6.INJ. NEOMOL 100ML IV/SOS ( IF TEMP > 101F)
7. IVF 5% D IF GRBS < 150MG/DL @ 75ML/HR.
1.IVF NS @ 150ML /HR.
2.INJ. 0.1 UNITS /KG/WT ACTRAPID IV/STAT.
3. INJ. PIPTAZ 2.25GM IV/TID.
4.INJ. ZOFER 4MG IV/SOS
5. INJ. PANTOP 30MG IV/OD.
6.INJ. NEOMOL 100ML IV/SOS ( IF TEMP > 101F)
7. IVF 5% D IF GRBS < 150MG/DL @ 75ML/HR.
ENT REFERAL WAS TAKEN IN VIEW OF RIGHT EAR DISCHARGE.
Icu bed : 1
S: PATIENT IN COMATOSED STATE.
O: PATIENT GCS : E2V1M3
PUPILS FIXED, NIT REACTING TO LIGHT
DOLLS EYE ABSENT
CORNEAL AND CONJUCTIVAL REFLEX ABSENT.
MOTOR POWER COULD NOT BE ELICITED
TONE DECREASED ON LEFT SIDE
REFLEXES
B. T. S. K. A. P
R. +2. +2. +1. -. -
L. +2. +2. +. - (amputated)
Tone - Left - hypotonia
Right -UL AND LL - NORMAL
TEMP: AFEBRILE
PR-103bpm
BP-90/60mmJg
Rr- 30cpm
P/A - soft, B SOUNDS +
R/S- crepts + in Right ICA, IMA, IAA (R>L).
CVS-S1 S2 +
A- DKA SECONDARY TO ? VIRAL PNEUMONIA WITH HYPOVOLAEMIC SHOCK SECONDARY TO DEHYDRATION WITH METABOLIC ACIDOSIS SECONDARY TO DA AND CKD RESOLVED WITH H/O DM II, CVA WITH S/P LEFT AMPUTATED LEG WITH ? SEPTIC ENCEPHALOPATHY WITH RIGHT EYE ORBITAL CELLULITIS WITH RIGHT EAR ASOM.
P- 1.IVF NS @ 150ML /HR.
2.INJ. 0.1 UNITS /KG/WT ACTRAPID IV/STAT.
3. INJ. PIPTAZ 2.25GM IV/TID.
4.INJ. ZOFER 4MG IV/SOS
5. INJ. PANTOP 30MG IV/OD.
6.INJ. NEOMOL 100ML IV/SOS ( IF TEMP > 101F)
7. IVF 5% D IF GRBS < 150MG/DL @ 75ML/HR
2D ECHO:
MRI:


LEFT MAXILLARY SINUSITIS, FLUID COLLECTION













Comments
Post a Comment